Guides/Tutorials
-
Searching the LiteratureEbling Library guide
-
EBP Tutorial Module 2: AcquireDuke University Medical Center Library & Archives
-
Finding the Current Best EvidenceChapter 5 from Users' Guide to the Medical Literature (3rd ed.)
-
Finding the EvidenceCentre for Evidence Based Medicine
-
PubMed: Finding the Best EvidenceEbling Library, 4:55 min.
Additional Reading
-
How to Read a Paper: Basics of Evidence-Based Medicine and Healthcare, 6th ed.Available online for UW students and staff
-
How to read a paperBMJ article series
-
How to perform an effective literature reviewSchwartz PB, Christensen L, Zafar SN. Am J Surg. 2022;224(3):1019-1022
-
Efficient literature searching: a core skill for the practice of evidence-based medicineDoig GS, Simpson F. Intensive Care Med. 2003;29(12):2119-2127. doi:10.1007/s00134-003-1942-5
-
Evidence-based practiceMcKibbon KA. Bull Med Libr Assoc. 1998;86(3):396–401
-
How to answer your clinical questions more efficientlyWeinfeld JM, Finkelstein K. Fam Pract Manag. 2005;12(7):37-41
-
Of studies, syntheses, synopses, summaries, and systems: the “5S” evolution of information services for evidence-based health care decisionsHaynes RB. ACP J Club. 2006;145(3):A8
Acquire the Evidence
Armed with our well-built clinical questions, clinicians proceed to identify and obtain an answer from the evidence found in the health literature. There are thousands of health information resources are currently available; therefore, an understanding of the essential value of each resource type is required to determine when each one can best be applied. Essentially, there are three general levels of literature:
Primary
Primary literature is where researchers publish their findings first. In the health field this is primarily in the form of journal articles outlining methodology, data, results, and conclusions. The evidence based approach emphasizes a hierarchy of evidence based on study types. When searching for single studies on a topic, clinicians should utilize database tools (limits and filters) to obtain the highest level of evidence to answer a clinical question. Examples: Randomized Controlled Trials, Cohort Studies, Case-Control Studies, Case Reports, Qualitative Studies
Secondary
Secondary literature summarizes the primary studies by appraising the relevant individual studies to answer a particular clinical question. In most cases, clinicians should initiate a search for answers to clinical questions with the secondary literature. Examples: Systematic Reviews, Meta-Analyses, Evidence-Based Guidelines, Some Clinical Database entries
Tertiary
There are now several online health information sources that accumulate the research (evidence) on clinical topics from the primary and secondary literature. These are often provide a very efficient way for clinicians to get up to speed on unfamiliar topics and filling holes in their knowledge base; however, clinicians should keep an eye on currency; the tertiary literature, by design, is lags behind the primary literature. Examples: Most guidelines and society statements, Most Clinical Database entries, Clinical Textbooks, Narrative Reviews
The Evidence Hierarchy
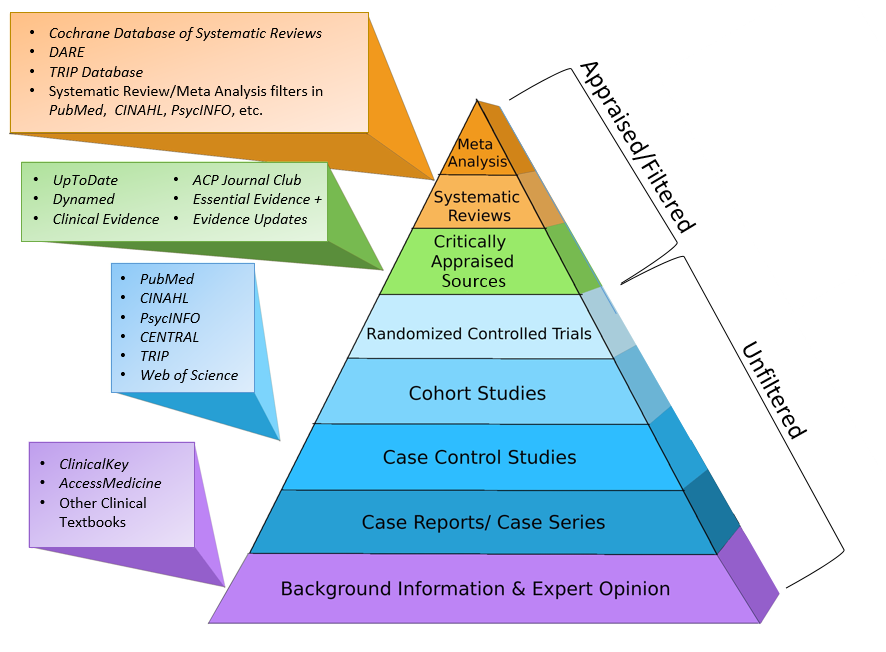
About the Hierarchy
The definition of EBM states the importance of obtaining the "best available evidence." The evidence hierarchy is an attempt to rank the health information resource/study designs with the highest quality sitting atop and the lower levels descending below. This hierarchy is helpful to guide evidence acquisition (literature searching) as well as providing clearer communication when discussing the landscape of health literature.
When it comes to prioritizing the evidence in any specific situation, clinicians will need understand the nuances of the evidence (reviews, studies) obtained. It is not uncommon for lower levels of evidence on the hierarchy to trump evidence sitting above: a hot-off the-press large RCT over an older meta analysis containing small studies.
Common Health Study Designs
Meta Analysis – type of systematic review that combines (pools) the results using accepted statistical methodology as if they were from one large study.
Systematic Review – focuses on a specific clinical question and includes an extensive/explicit review of the literature to identify studies with sound methodology. Data extracted from the selected studies are combined (if possible), compared, and assessed. Conclusions are made based on results and/or the presence or absence of supporting evidence.
Randomized Controlled Trial (RCT) – prospective, analytical, experimental study using data obtained in the clinical environment. Individuals similar at the beginning are randomly allocated into treatment groups and outcomes are compared after sufficient follow-up time. A study that shows the efficacy of a diagnostic test is a prospective, blind comparison to a gold standard. This is a controlled trial that looks at individual with varying degrees of an illness and applies diagnostic tests to each individual: the test under investigation and the “gold standard” test.
Cohort Study – prospective, analytical, observational study of a population (or cohort) who had, have or will have a specific exposure or treatment of interest. The outcome of the cohort is compared to the general population or another group that has not been exposed to exposure or treatment of interest. Cohort studies are susceptible to bias because the two groups may differ in ways beyond the variable in the study.
Case-Control Study – retrospective, analytical, observational study based on secondary data in which individuals with a condition or outcome are compared with individuals who do not, but have the same risk factor. Often using medical records or patient recall, researches look back in time to identify possible exposures. Very useful for rare conditions or for risk factors with long induction. Due to potential bias, case control studies provide relatively weak empirical evidence even when properly executed.
Case Series/Case Report – anecdotal evidence. A description of a single case (or several cases), typically describing the manifestations, clinical course, and prognosis of that case. Due to the wide range of natural biologic variability in these aspects, a single case report provides little empirical evidence to the clinician. They do describe how others diagnosed and treated the condition and what the clinical outcome was
-
Study designsCEBM Oxford
-
Introduction to study designCEBM Oxford